Tesamorelin is a synthetic peptide analog of the naturally occurring human Growth Hormone-Releasing Hormone (GHRH). Unlike GHRPs (like Ipamorelin or GHRP-6), which stimulate GH release through the ghrelin receptor, Tesamorelin functions as a true GHRH analog, binding directly to the GHRH receptor on the pituitary gland to stimulate the pulsatile release of endogenous growth hormone.
Key Research Focus
- Visceral Adipose Tissue (VAT): tesamorelin is most notably studied for its ability to reduce visceral fat, specifically in individuals with HIV-associated lipodystrophy.
- Cognitive Function: Emerging research is investigating the potential neuroprotective effects of GHRH analogs in mild cognitive impairment and age-related memory decline.
- Metabolic Health: Due to its impact on IGF-1 levels, it is frequently studied for its role in muscle body composition management and lipid metabolism.
Tesamorelin (Egrifta SV) is the only FDA-approved GHRH analog, indicated for visceral fat reduction in HIV-associated lipodystrophy. CJC-1295 is a research-only GHRH analog available in two forms: with DAC (half-life 6-8 days) and without DAC (half-life ~30 minutes). In Phase III clinical trials, tesamorelin reduced visceral adipose tissue by 18% (-34 cm2) over 6 months (Stanley et al., JAMA, 2014). CJC-1295 increased GH 2-10-fold and IGF-1 1.5-3-fold in a Phase I study of 21 subjects (Teichman et al., J Clin Endocrinol Metab, 2006). The key difference: tesamorelin has Phase III clinical trial data; CJC-1295 has Phase I/II data only.
Technical Specification Table
| Feature | Description |
|---|---|
| Peptide Name | Tesamorelin Acetate |
| Chemical Formula | C221H366N72O67S · x(C2H4O2) |
| Classification | GHRH Analog |
| Mechanism | Stimulates pituitary GHRH receptors |
| Molecular Weight | ~5135.9 g/mol (Base) |
| Quick Reference | Tesamorelin | CJC-1295 (With DAC) | CJC-1295 (No DAC) |
|---|---|---|---|
| FDA status | Approved (NDA 022505) | Not approved | Not approved |
| Indication | HIV-associated lipodystrophy | Research only | Research only |
| Half-life | 26-38 minutes | 6-8 days | ~30 minutes |
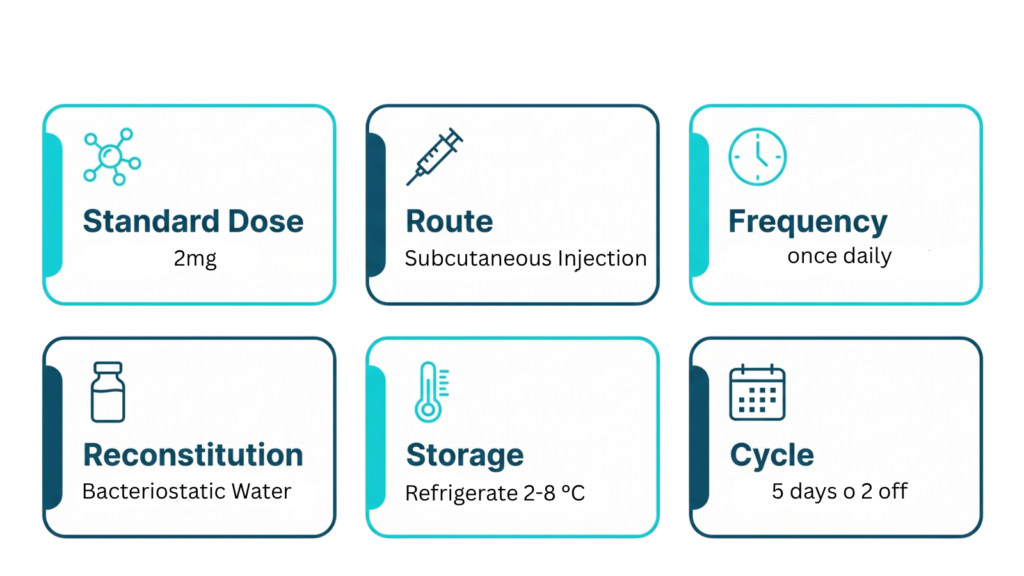
| Dosing | 2 mg daily (subcutaneous) | 1-2 mg weekly | 100-200 mcg, 2-3x daily |
| Clinical evidence | Phase III RCTs (JAMA, NEJM) | Phase I/II | Phase I/II |
Tesamorelin: Phase III Randomized Controlled Trials
The Stanley 2014 JAMA study enrolled subjects with HIV-associated lipodystrophy and measured visceral adipose tissue (VAT) by CT scan. Tesamorelin at 2 mg/day produced a mean reduction of 34 cm2 in VAT over 6 months. It also reduced liver fat and improved triglyceride levels (Stanley et al., JAMA, 2014).
The Falutz 2007 NEJM study enrolled 412 subjects in a randomized, double-blind, placebo-controlled trial. Tesamorelin produced a 15.2% decrease in VAT and reduced triglycerides by approximately 50 mg/dL. Among treated subjects, 69% met the FDA responder threshold of greater than 8% VAT reduction (Falutz et al., NEJM, 2007).
Fourman et al. (2012) showed that VAT responders had significantly improved triglycerides and adiponectin levels, connecting fat reduction to broader metabolic improvement (Fourman et al., 2012).
| Tesamorelin Trial | N | Design | Key Result |
|---|---|---|---|
| Stanley 2014 (JAMA) | 48 | RCT, double-blind | -34 cm2 VAT, liver fat reduction |
| Falutz 2007 (NEJM) | 412 | RCT, double-blind | -15.2% VAT, -50 mg/dL triglycerides |
| Falutz 2008 (extension) | 273 | 52-week open-label | Sustained benefit at 1 year |
How to Reconstitute Peptides Step by Step
- Insert the needle through the stopper and inject the water slowly down the inside wall of the vial. Do not aim directly at the powder.
- Clean the rubber stopper of your peptide vial with an alcohol swab and let it dry.
- Using a syringe, draw the calculated amount of bacteriostatic water.
- Gently swirl the vial until the powder dissolves completely. Never shake it, as this can degrade the peptide.
- Store the reconstituted vial in your refrigerator (2-8 °C). Use within 3 to 4 weeks.
Q: How does Tesamorelin differ from CJC-1295?
A: While both are GHRH analogs, CJC-1295 is modified to have a longer half-life (especially the DAC version). Tesamorelin is a specific analog that has been clinically validated for its efficacy in reducing visceral adipose tissue in specific metabolic conditions.
Q: Is it FDA approved?
A: Yes, Tesamorelin (under the brand name Egrifta) is FDA-approved for the treatment of excess visceral fat in patients with HIV-associated lipodystrophy. However, usage outside of this specific indication is considered off-label and remains within the realm of investigational research.
Q: Does it increase appetite like ghrelin mimetics?
A: Generally, no. Because Tesamorelin acts on the GHRH receptor rather than the ghrelin receptor, it typically does not cause the significant increase in hunger often associated with GHRP-6 or Ipamorelin.
Q: Does Tesamorelin reliably elevate IGF-1 levels?
A: Yes. One of the primary biomarkers used in clinical studies to verify Tesamorelin efficacy is the rise in Insulin-like Growth Factor 1 (IGF-1). Because Tesamorelin stimulates the pituitary to release growth hormone, the subsequent hepatic production of IGF-1 is typically elevated in a dose-dependent manner.
Q: What is the optimal storage protocol for reconstituted Tesamorelin?
A: Once reconstituted with bacteriostatic water, the peptide is highly prone to degradation. It must be stored in a refrigerator (typically 2°C–8°C) and is generally recommended for use within a short window (often 7–14 days) to maintain its structural integrity. Avoid freezing the reconstituted solution.
Q: Why is consistent dosing time considered important in research?
A: Tesamorelin is researched for its ability to restore pulsatile growth hormone secretion. Maintaining consistent administration timing—often in the morning on an empty stomach—is intended to align with the body’s natural circadian rhythm of growth hormone release, potentially optimizing the physiological response.
Q: Is there any risk of “desensitization” with long-term use?
A: In clinical settings, long-term administration has been studied. However, research models often implement “cycling” (e.g., 5 days on, 2 days off, or alternating month-long protocols) to mitigate the potential for receptor downregulation and to allow the pituitary gland to maintain its sensitivity to the exogenous GHRH analog.
Conclusions
Among those with clinically significant decrease in visceral adipose tissue on treatment, tesamorelin was effective in increasing skeletal muscle area and density. Long term effectiveness of tesamorelin among people with and without HIV, and the impact of these changes in daily life should be further studied.
| Resource | Description | Link |
|---|---|---|
| PubMed | Peer-reviewed research and clinical studies. | View Studies |
| ClinicalTrials.gov | Active and completed clinical trial records. | View Trials |
| PubChem | Chemical properties and molecular data. | View Data |
| FDA (Drugs@FDA) | Official prescribing information and labels. | Search FDA Data |
Our Recommended UK Supplier
Tesamorelin is available from Peptronic Labs UK-based, ≥99.0% purity verified by HPLC, Royal Mail Tracked 24 View Tesamorelin


